

The Most Preventable Dangerous Call in EMS?
This article is the 4th installment in a 7-part series on EMS patient refusal implementation and documentation. Each article will take a look at one specific area of refusal documentation and how to best execute a patient refusal and document the interaction in a legally defensible manner.
Part 4. Failure to Contact Medical Control on High-Risk Refusals
By Paul Girard & Kevin Kelley
In this installment we’re going to talk about one of the most avoidable mistakes we see in refusal documentation: a high-risk refusal where the crew never contacts online medical control (OLMC). This isn’t about “checking a box.” It’s about patient safety, provider decision-making, and whether your chart can withstand the bright light of hindsight, QA/QI review, and litigation discovery when the outcome goes bad.
Example:
You are dispatched for “difficulty breathing.” The patient is sitting upright on the couch, talking in full sentences, and insists it’s “just a panic attack.” The spouse is worried. You get a set of vitals that are not reassuring, but the patient keeps repeating, “I’m not going to the hospital.” You try the standard counseling. The patient signs. You clear.
Six hours later the tones drop again for the same address—this time “unresponsive.” Now everyone has questions: What did you think it was? What did you tell the patient? Did they understand the risk? Did you follow your refusal policy? And one question tends to rise to the top fast: did you contact OLMC when you realized this was not a routine refusal? That question matters because it sits at the intersection of patient safety and defensibility—and it’s exactly where high-risk refusals live.
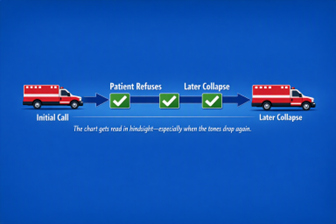
FIGURE 1: The Second‑Dispatch Problem
The PCR gets read in hindsight—especially when the tones drop again for the same address.
Patients frequently make decisions based on how they feel in the moment. EMS providers must explain that the concern is not only what is visible, but what may be hidden beneath the surface. If this uncertainty is not explained, the refusal is not fully informed.
What makes a refusal “high risk”?
Not every refusal is created equal. A patient declining transport after a minor complaint with normal vital signs and a clearly benign story is one thing. A patient declining transport when the presentation is time-sensitive, the vital signs are abnormal, the story doesn’t add up, or the patient’s ability to understand the risks is questionable is a different animal entirely. That second category is what we mean by “high risk.”
High-risk refusals tend to share a common theme: there is a meaningful possibility of deterioration, disability, or death if the patient delays definitive evaluation and treatment. They also tend to be the cases where the chart is more likely to get read by people who were not there—CQI reviewers, medical directors, regulators, plaintiff attorneys—and they will all ask the same question: “Why didn’t anyone try harder to convince the patient to be seen?”

Figure 2: Abnormal Vital Signs
Abnormal vital signs + refusal is where “routine” quietly becomes high risk
What it means when you don’t contact OLMC
Operationally, “failure to contact OLMC” usually means one of two things: (1) your protocols clearly required consultation and it never happened, or (2) the situation was clinically concerning enough that a reasonable paramedic would have reached out for a second opinion, a physician voice, or both, and the crew decided to go it alone.
Either way, you’ve lost an important safety net. And just as importantly, you’ve lost contemporaneous medical oversight documentation that can help demonstrate you recognized the risk, escalated appropriately, and made a thoughtful attempt to protect the patient from the consequences of a bad decision. With that foundation, let’s talk about what can go wrong.
Patient safety perils: the rescue opportunity you didn’t take
When we audit refusals, we’re not looking for perfection—we’re looking for reasonable, defensible steps that improve patient safety. Contacting OLMC on the right refusal is one of the simplest high-value moves you can make. When you skip it, you often lose the best chance you had to “rescue” the patient from a dangerous refusal.
The “fresh voice” effect
Patients don’t always hear risk the same way from the same person. They may be embarrassed, defensive, intoxicated, frightened, or simply dug in. A physician—especially one who is calm, direct, and clearly focused on the patient’s welfare—can sometimes break through where field persuasion stalls. When you don’t make that call, you’re betting the patient’s outcome on your ability to convince them in the moment, without backup.
Capacity isn’t a check mark
Capacity is task-specific and it is not guaranteed just because the patient can state their name and the date. Hypoxia, hypoglycemia, intoxication, head injury, shock, psychiatric crisis, and severe pain can all quietly degrade a patient’s ability to understand, weigh, and communicate a rational choice. OLMC can provide a “second set of eyes” on the question of capacity and can help guide you toward additional assessment steps that strengthen your clinical and legal footing.
Safer alternatives don’t appear by accident
Some refusals don’t convert to transport, even with your best effort. But there is a wide gap between “refused transport” and “we left.” OLMC can help you think through options that reduce harm: repeat vital signs, targeted diagnostics (like glucose or a 12-lead), involving a caregiver, arranging alternate transport, or very clear return precautions and re-contact plans. The patients who get in trouble after a refusal are often the ones who were given a binary choice—go with us or sign here—without a structured plan for what happens next. Online control can help create a structured plan that can lead to minimizing bad outcomes.
Dynamic scenes turn into static charts
Refusal scenes are messy. People argue. Families negotiate. Symptoms wax and wane. Then, days later, the event is reduced to a few paragraphs in a PCR. If the patient decompensates after you leave, that PCR becomes the story. When there is no OLMC contact, the record reads like the crew made a unilateral decision to accept the refusal and clear the scene, even if that is not how it happened in real time.
Clinical perils: anchoring, normalization, and the illusion of “fine”
High-risk refusals are fertile ground for cognitive traps. Crews are under time pressure, the patient is minimizing, and the presentation may be subtle. Without escalation, it is easy to slide into anchoring: “It’s anxiety.” “It’s indigestion.” “They always refuse.” “They look fine now.”
The problem with “fine” is that it’s not a diagnosis. Field assessment can be reassuring without being definitive, and normal or near-normal findings do not rule out life threats. OLMC consultation forces a pause. It forces you to present the case, say the vital signs out loud, articulate your concern, and hear another clinician challenge—or confirm—your thinking. That pause alone can prevent a bad miss.
It also reduces the chance you miss protocol-driven refusal triggers. If your guidelines call for OLMC based on complaint category, age, abnormal vitals, anticoagulant use, altered mental status, or other red flags, failing to call doesn’t just increase clinical risk—it creates an obvious, documentable deviation from expected practice.
Legal and regulatory perils: an easy-to-prove breach
In the refusal world, the legal analysis is often brutally simple. First: did the crew recognize the risk and take reasonable steps to protect the patient? Second: did the crew follow their own protocols? When OLMC is required—or clearly indicated—and it doesn’t happen, you hand an investigator or plaintiff attorney an “easy button.” They don’t have to argue about subtle clinical nuances. They can point to a missing safety step that would have taken only a few minutes to perform.
And remember: high-risk refusals are disproportionately represented in QA/QI and in discovery because bad outcomes bring scrutiny. When the outcome is poor, everyone will replay the call with the benefit of information you did not have in the moment. Your only protection is the reasonableness of your actions and the quality of your documentation.
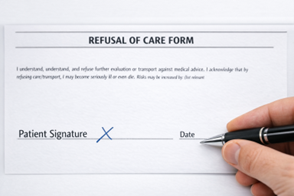
Figure 3: Patient Signature
A signature is not a shield if capacity, risk, and alternatives aren’t clearly documented.
Documentation vulnerabilities multiply fast
When you skip OLMC, you lose more than medical input. You lose corroboration. A well-documented OLMC contact—time, physician name, key recommendations, and the patient’s response—helps show you escalated appropriately and that the patient was warned in a serious, unmistakable way.
Without that, the chart is more vulnerable to the classic post-event critiques: “They didn’t take it seriously.” “They didn’t explain the risk.” “They were in a hurry.” Even if those statements are unfair, your documentation has to be strong enough to refute them.
Communication perils: credibility, conflict, and mixed messages
Refusals are often less about medicine and more about human behavior. Patients refuse because of fear, cost, pride, intoxication, fatigue, immigration concerns, bad prior experiences, or the simple belief that “this will pass.” When tension rises, a physician voice can de-personalize the disagreement. It shifts the conversation from “the paramedic wants to take me” to “a doctor is telling me the risk is real.” Lets face it, for many people a physician opinion will hold more weight than other people’s opinion, even an experienced medics.
OLMC also helps prevent the “committee refusal,” where family, bystanders, fire, and law enforcement all weigh in with different opinions. Inconsistent messaging confuses patients and weakens your leverage. One clear medical authority statement—properly documented—often simplifies the scene.
System perils: repeat calls, sentinel events, and reputational damage
High-risk refusals have a way of coming back to haunt agencies. The patient calls again. The family files a complaint. The hospital sees the patient later in extremis. Then the case becomes a CQI review, a morbidity and mortality discussion, a regulator inquiry, or a lawsuit.
From a risk-management perspective, “abnormal vital signs + refusal + no OLMC contact” is a pattern that practically advertises itself. It’s the kind of chart that makes medical directors ask hard questions and makes agencies scramble to defend decisions that could have been supported by a simple phone call.
There are also downstream costs: corrective action, remediation, strained relationships with the base station, increased insurance exposure, and the time sink of investigations and interviews. None of that helps patients, and none of it helps crews.
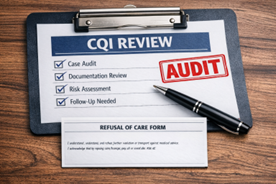
Figure 4: CQI Review
High‑risk refusals are disproportionately represented in QA/QI reviews, audits, and adverse‑outcome investigations.
Why providers don’t contact medical control
When conducting CQI audits, we frequently speak with field providers regarding the need for online medical control. Reasons for not contacting control vary but often fall into one or more of 3 categories:
- I didn’t think I needed to
- Why bother, it takes way too long to do that and we only get a cursory response to the request (sometimes summarized as, “if they want to refuse let them refuse, why are you bothering me”)
- They give us push-back when we call and tell us we are bothering them and often make providers feel guilty for having called
The first excuse can often be tricky as many refusal protocols are vague and can be open to interpretation as to what constitutes a “high risk” refusal. Some providers may even argue with you about whether the protocol is supportive of the need for online control. In some cases, you may even need to get clarity from the service medical director for his/her opinion on how to interpret individual cases.
The second and third excuse more often has to do with whether the providers feel they have support from online control. It can also be an indication of simple laziness on the part of the provider. Either way, when these instances arise, it is imperative that the CQI officer reinforce that even if the person on medical control is not helpful or even off-putting, your job as an EMS provider is to do what is required of you and do not let whoever is answering that phone or radio at the receiving facility dictate how you will do your job. Especially if they are trying to get you to perform in a way that violates your requirements.
This type of response should also be brought to the attention of management so it can be rectified, not simply ignored. We also try to help the provider understand that by not calling medical control for these reasons, they are assuming significant risk on themselves. If they did not try to obtain medical control when they were supposed to, that is on the provider. If medical control is attempted and is unhelpful, that is on medical control.
What “good” looks like: a practical standard for the field
The goal is not to call OLMC on every refusal. The goal is to call when the refusal is high risk, when protocols require it, when you’re unsure about capacity, or when something in your gut says, “If this goes bad, this is going to be ugly.” That intuition is often your experience recognizing a pattern before your brain has fully named it.
When to call
If your protocol mandates OLMC, the decision is already made—call. If it doesn’t, but the patient has red flags (abnormal vitals, concerning complaints, extremes of age, altered mental status, anticoagulation, significant comorbidities, unreliable history, or a concerning exam), call anyway. High-risk refusals are precisely what OLMC is for.
How to call (and how to use the call)
Keep it concise: chief complaint, relevant history, assessment findings, vital signs (including trends), what you believe the risk is, and exactly what the patient is refusing. Then ask for what you need—guidance, a second opinion, or a physician-to-patient conversation to reinforce the seriousness of the situation.
What to document
Document your capacity assessment in plain language and document the patient’s understanding. A simple “teach-back” is powerful: have the patient explain, in their own words, what you told them could happen and what they plan to do if symptoms worsen.
Then document the OLMC contact: physician name (or identifier per policy), time, key recommendations, and the patient’s response. Finally, document the alternatives discussed and explicit return precautions. If the patient still refuses, your documentation should show a thoughtful, escalated, safety-focused process—not a quick signature and a quick exit.
Closing Thoughts
In a high-risk refusal, OLMC is not a burden—it’s a tool. It protects the patient by increasing the odds they make a safer decision. And it protects the provider and the agency by showing that when the stakes were high, you escalated, you communicated risk clearly, and you did not treat a dangerous refusal like routine paperwork. The risk is poor patient outcomes, agency and provider reputations ruined, or career disruption or even career ending, and as we stated in the title, a risk to an EMS providers life, liberty, and pursuit of happiness
¨¨¨¨¨¨
If your organization needs help with patient refusal documentation, contact us for a quote to create a custom program for you.
You can also check out our introductory article on this topic: Patient Refusals: A Risk to an EMS Providers Life, Liberty, and Pursuit of Happiness
Or Part 1 in the series: Incomplete Patient Assessment
Part 2 in the series: Missing Signatures and Incomplete Refusal Forms
Part 3 in the series: Poorly Explained Risks of Refusing
For more information you can visit the Girard & Associates website at www.girardassoc.com or contact Paul Girard at paul.girard@girardassoc.com or Kevin Kelley at kevinkelleylaw@gmail.com.
About the Authors
Paul Girard, a retired paramedic and EMS Director, is the Founder and President/CEO of Girard & Associates, Inc., a national EMS clinical quality improvement consulting firm. He has worked in EMS continuous quality improvement since the mid-1980s and founded Girard & Associates, Inc. in 2005 to help EMS agencies better monitor, evaluate, and improve the patient care they provide. An EMS CQI entrepreneur, Paul invented and utilizes a proprietary scoring and rating system that drives a teaching, coaching, and mentoring-based CQI process, supporting providers in strengthening clinical judgment, documentation quality, and professional performance. The firm delivers CQI auditing, program development, and CQI program administration for EMS agencies nationwide. Paul is also the co-host of “The G&A Way EMS CQI” podcast.
Kevin J. Kelley, Esq. began his EMS career in 1986. A retired paramedic and EMS Director turned attorney in 2004, Kevin is the founder of Rescuing Rescuers, PLLC, a Massachusetts law firm dedicated to representing firefighters, EMTs, paramedics, and other licensed healthcare professionals. His practice focuses on EMS license regulatory defense, on- and off-duty criminal and self-defense matters, clinical documentation risk assessment, and firehouse EMS-focused education designed to strengthen patient safety, provider decision-making, and professional defensibility before DPH/OEMS, Division of Administrative Law Appeals, and civil and criminal courts. Kevin is also the co-host of “The G&A Way EMS CQI” podcast.


{kind=link}
{kind=link}
{kind=link}