

The Most Preventable Dangerous Call in EMS?
This article is the 3rd installment in a 7-part series on EMS patient refusal implementation and documentation. Each article will take a look at one specific area of refusal documentation and how to best execute a patient refusal and document the interaction in a legally defensible manner.
Part 3. Risks of Refusal Not Properly Explained
By Paul Girard & Kevin Kelley
One of the most common weaknesses in EMS refusal cases is also one of the easiest to overlook: the risks of refusing care are not properly explained, or not properly documented. Providers often believe they covered this step. When the EMS patient care report (PCR) is reviewed later, the documentation frequently does not support that conclusion.
For example, in Massachusetts, the Statewide Treatment Protocol 7.5 is clear. It states:
“A patient must be fully informed about his or her medical condition, the risks and benefits associated with the proposed treatment and the risks associated with refusing care.”
The protocol further instructs providers to:
“Explain to the patient the nature and severity of his/her illness or injury, the treatments being proposed, the risks and consequences of accepting or refusing treatment, and the potential alternatives. Fully document the explanation given to the patient in your trip report.”
This is the standard. If the explanation is vague, generic, or poorly documented, the refusal becomes difficult to defend. In fact, it may not be a patient refusal at all.
Most states have some standardized language in EMS regulation requiring field providers to adequately assess and try to convince the patient to be seen at a medical facility as opposed to refusing care in the field. This is prudent as there are serious limitations for field providers in their ability to assess patients completely enough to rule out some serious conditions in the field.
EMS personnel are trained to assess for potentially life-threatening injury or illness that requires immediate attention. They are not trained for every conceivable medical condition a patient may have. Other parts of the medical system are designed for more in-depth medical assessments and treatments that may potentially benefit a patient.
The Iceberg Concept: What You Don’t See Matters Most
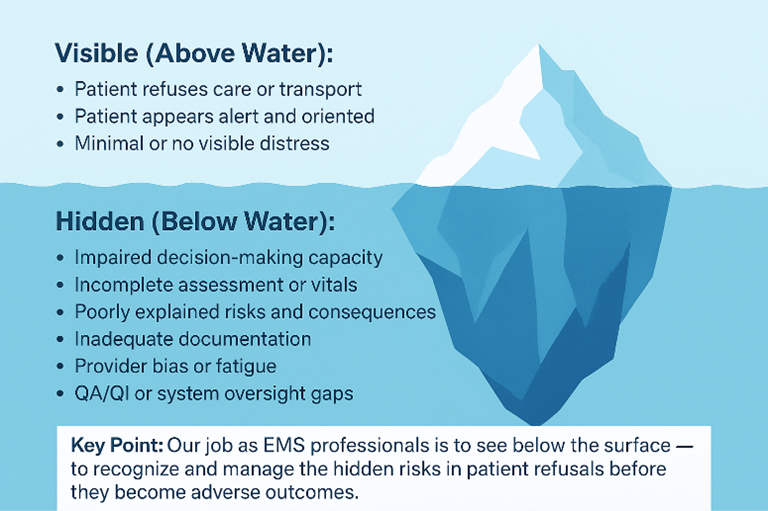
A useful way to think about refusal risk is the iceberg concept. What EMS sees on scene is often only the visible portion of the problem. The patient’s complaint, appearance, and initial vital signs represent what is above the surface.
Beneath the surface may be developing pathology that is not yet obvious.
A patient with dizziness may appear stable but could be experiencing stroke, arrhythmia, dehydration, infection, medication interaction, or intracranial pathology. A fall that appears mechanical may actually be caused by syncope or underlying medical instability. Shortness of breath may represent an evolving process that has not fully declared itself.
Patients frequently make decisions based on how they feel in the moment. EMS providers must explain that the concern is not only what is visible, but what may be hidden beneath the surface. If this uncertainty is not explained, the refusal is not fully informed.
The Swiss Cheese Model and Refusal Safety
Safety science offers another way to understand why risk explanations matter. The Swiss Cheese Model, described by James Reason, explains that adverse events occur when multiple layers of protection fail at the same time.
Each layer of care acts as a safeguard. In refusal encounters, those layers include:
- assessment
- vital signs
- capacity evaluation
- risk explanation
- documentation
- medical control consultation when indicated
Each layer has weaknesses. No single step is perfect. However, when multiple weaknesses align, the patient can fall through the system.
The risk explanation is one of those layers. If it is weak or generic, the patient may not understand the potential seriousness of their condition. If that weakness aligns with incomplete assessment, missing vital signs, or rushed documentation, the refusal becomes unsafe.

In other words, a poor risk explanation does not always cause harm by itself. But when combined with other deficiencies, it removes a critical safeguard.
What “Fully Informed” Means
A proper risk explanation is not a generic warning. It must be tied to the patient’s presentation. The discussion should include:
- what EMS believes may be occurring
- why evaluation is recommended
- what could happen if the patient stays home
- what benefits evaluation may provide
- what alternatives exist
- what the patient says in response
Statements such as “patient advised of risks” or “patient aware they could die” are conclusions. They do not show what was actually explained.
Specific explanations demonstrate that the provider connected the assessment to real risk.
Avoiding Generalized Language
Generic phrases weaken refusal documentation. Examples include:
“Patient advised of all risks including death.”
“Patient refused against medical advice.”
“Patient aware of risks.”
These statements do not show meaningful discussion. They do not demonstrate that the patient actually understood their situation.
A stronger narrative ties risks to the patient’s condition. For example, documenting that symptoms could represent a cardiac issue, stroke, infection, or other serious condition shows that the explanation was individualized.
The goal is not to alarm the patient. The goal is to ensure that the patient understands that what appears minor may not be minor.
Explaining Benefits
In Massachusetts, STP 7.5 requires explaining both risks and benefits. Patients should understand what further evaluation could provide, including:

- Diagnostic testing
- monitoring
- imaging
- laboratory work
- observation
- specialist consultation
- evaluation by a higher trained medical provider (i.e. a physician at the ED)
This helps patients understand what they are declining. It also strengthens documentation that the decision was informed.
Discussing Alternatives
Alternatives should also be explained. Some examples may include:
- transport by ambulance
- transport by private vehicle
- urgent care evaluation
- follow up with primary care
- calling EMS again if symptoms change
Documenting alternatives demonstrates that the patient was given reasonable choices. Providers must remember, however, that the risks of alternatives also need to be explained to the patient and fully documented.
Field Assessments Are Limited
It is appropriate to explain that EMS field assessments are limited. EMS does not have access to imaging, laboratory testing, or extended monitoring. A patient who appears stable may still have an underlying condition.
This reinforces the iceberg concept. It communicates that EMS cannot rule out all serious causes.
The Patient’s Response
The patient’s response should be documented. This demonstrates understanding. Including the patient’s own words strengthens the narrative.
Examples include:
- Patient states symptoms have improved and prefers follow up with primary care.
- Patient acknowledges risk of worsening condition but declines transport.
- Patient verbalizes understanding that condition could deteriorate.
- Patient still refuses transport stating they have had bad experiences in hospitals and will never go back, received a big bill, etc.
This shows participation in the decision-making process.
Advising the Patient They Can Call Back
Patients should be advised that they can call back if their condition changes. Documenting this shows that EMS encouraged further care and did not steer the patient toward refusal.
This supports the conclusion that the refusal was patient initiated.

Risk Explanation and Capacity
Risk explanation is closely tied to capacity. A patient cannot make an informed decision without understanding risks. If the patient cannot explain the risks in their own words, capacity may be questionable. While you may explain the risks of refusing in detail, if the patient does not understand what you are telling them, the refusal is not informed.
Patients may not understand the significance of what you are trying to tell them due to a variety of reasons including lack of understanding of medical terminology, an altered mental state, or language barriers for example. You must be able to prove through your documentation that any barriers to understanding were overcome by prudent actions on your part. Having the patient explain to you what you just stated to them helps to show there were no barriers to understanding.
Documenting understanding supports both the capacity determination and the refusal.
Scene Time and Risk Explanation
Meaningful risk explanations take time. Very short scene times often correlate with weak documentation. This does not mean refusals must be lengthy, but meaningful discussion must occur. We often see refusal reports where the on-scene time is 4 or 6 minutes. In all likelihood, this was not a properly executed refusal and even a layperson can conclude that EMS did not perform all the necessary steps to account for an informed refusal process.
When documentation is minimal or on scene times excessively short, reviewers may conclude that the conversation was rushed and not as complete as required.
Why Risk Explanations Fail
Risk explanations often fall short due to:
- time pressure
- fatigue
- assumption that the condition is minor
- patient impatience
- family pressure
- normalization of shortcuts
- provider laziness
These factors are common. They do not change the requirement that refusals must be informed.
Documentation Is Critical
The explanation must be fully documented. This includes:

- What was explained
- what risks were discussed
- what benefits were discussed
- what alternatives were offered
- what the patient said
- what the patient decided
If documentation is minimal, reviewers assume the explanation was minimal.
The Bottom Line
Failure to properly explain the risks of refusal is one of the most common weaknesses in EMS documentation. The iceberg concept reminds us that what appears minor may conceal serious pathology. The Swiss Cheese Model shows that when multiple safeguards fail, harm becomes more likely.
Risk explanation is one of those safeguards. When it is weak, a critical layer is removed.
Providers must explain the nature of the condition, the risks of refusing care, the benefits of evaluation, and the alternatives available. That discussion must be documented thoroughly.
Clear, specific risk explanations support informed decision making and strengthen defensibility. Generic statements do not.
In refusal cases, what lies beneath the surface matters. The PCR should demonstrate that the patient understood the risks of treatment and transport before deciding to remain at home.
An uninformed patient refusal is not a patient refusal at all. It is a risk to the safety of the patient, EMS provider, and EMS agency.
¨¨¨¨¨¨
If your organization needs help with patient refusal documentation, contact us for a quote to create a custom program for you.
You can also check out our introductory article on this topic: Patient Refusals: A Risk to an EMS Providers Life, Liberty, and Pursuit of Happiness
Part 1 in the series: Incomplete Patient Assessment: The Most Common Risk to the Patient, EMS Provider, and Agency
Part 2 in the series: Missing Signatures and Incomplete Refusal Forms: The Most Common Risk to the Patient, EMS Provider, and Agency
For more information you can visit the Girard & Associates website at www.girardassoc.com or contact Paul Girard at paul.girard@girardassoc.com or Kevin Kelley at kevinkelleylaw@gmail.com.
About the Authors
Paul Girard, a retired paramedic and EMS Director, is the Founder and President/CEO of Girard & Associates, Inc., a national EMS clinical quality improvement consulting firm. He has worked in EMS continuous quality improvement since the mid-1980s and founded Girard & Associates, Inc. in 2005 to help EMS agencies better monitor, evaluate, and improve the patient care they provide. An EMS CQI entrepreneur, Paul invented and utilizes a proprietary scoring and rating system that drives a teaching, coaching, and mentoring-based CQI process, supporting providers in strengthening clinical judgment, documentation quality, and professional performance. The firm delivers CQI auditing, program development, and CQI program administration for EMS agencies nationwide. Paul is also the co-host of “The G&A Way EMS CQI” podcast.
Kevin J. Kelley, Esq. began his EMS career in 1986. A retired paramedic and EMS Director turned attorney in 2004, Kevin is the founder of Rescuing Rescuers, PLLC, a Massachusetts law firm dedicated to representing firefighters, EMTs, paramedics, and other licensed healthcare professionals. His practice focuses on EMS license regulatory defense, on- and off-duty criminal and self-defense matters, clinical documentation risk assessment, and firehouse EMS-focused education designed to strengthen patient safety, provider decision-making, and professional defensibility before DPH/OEMS, Division of Administrative Law Appeals, and civil and criminal courts. Kevin is also the co-host of “The G&A Way EMS CQI” podcast.



{kind=link}
{kind=link}
{kind=link}